Free North Dakota Ems Patient Care Report PDF Form
Free North Dakota Ems Patient Care Report PDF Form
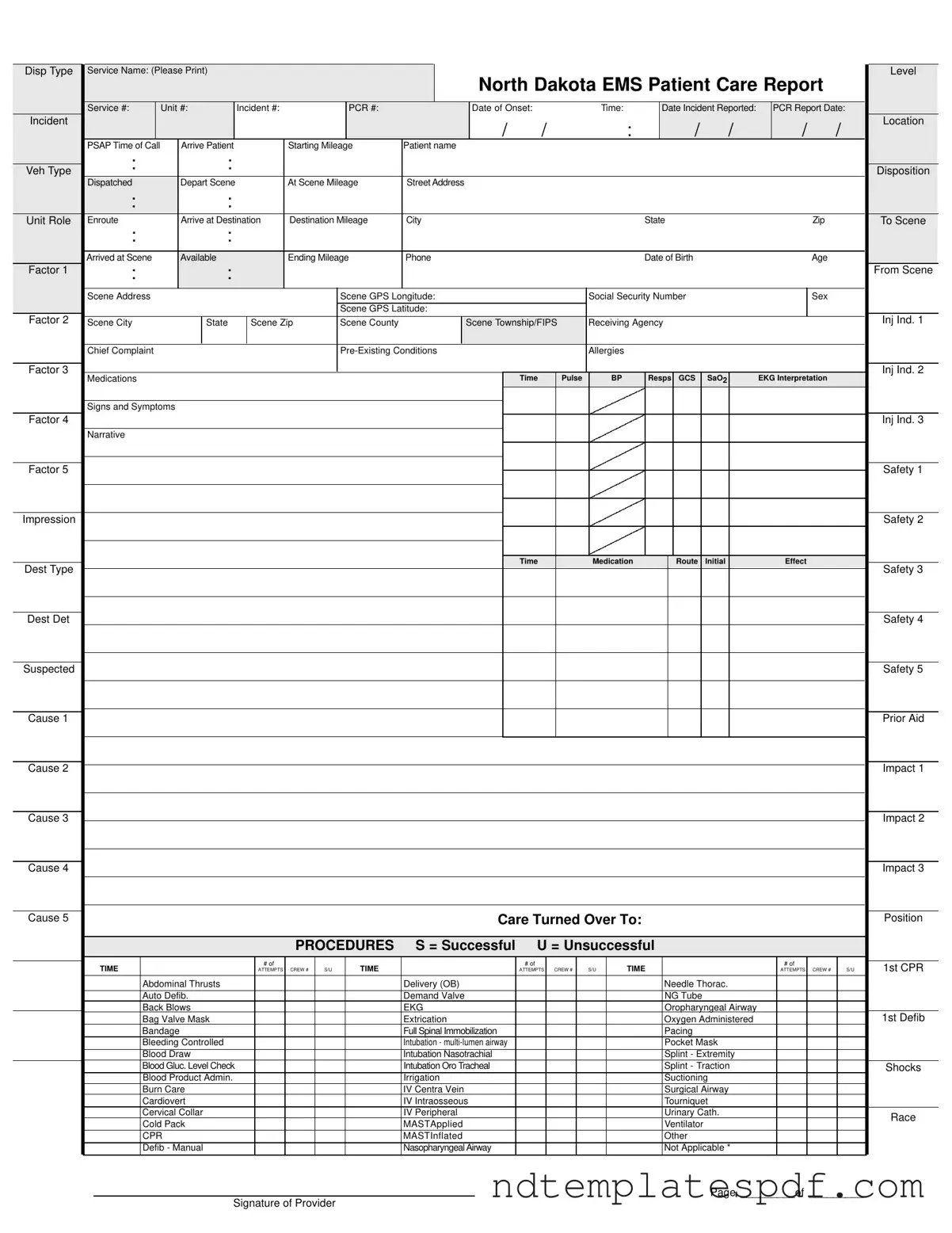
When filling out the North Dakota EMS Patient Care Report form, there are several key points to keep in mind to ensure accuracy and compliance.
| Fact Name | Description |
|---|---|
| Form Purpose | The North Dakota EMS Patient Care Report form is used to document patient care provided during emergency medical services. |
| Governing Law | This form is governed by North Dakota Century Code § 23-27-01, which outlines the requirements for EMS documentation. |
| Required Information | Essential details include patient demographics, incident specifics, and the care provided during transport. |
| Billing Information | The form includes sections for insurance details and responsible party information for billing purposes. |
| Signature Requirement | Patient signatures are required to acknowledge receipt of services and to consent to treatment or refuse it. |
Mental Health Involuntary Commitment - Submitting the form allows the Office of Attorney General to begin the approval process efficiently.
For individuals seeking to present their best qualities, a well-crafted Recommendation Letter can be invaluable. By utilizing the professional template for a Recommendation Letter, candidates can effectively convey their skills and experiences, making a significant impact on potential employers or admissions committees.
North Dakota Nonresident Filing Requirements - If total payments are less than taxes due, the balance due is calculated on line 14.
When filling out the North Dakota EMS Patient Care Report form, attention to detail is critical. Here are six important do's and don'ts to ensure accuracy and compliance:
Completing the North Dakota EMS Patient Care Report form is essential for documenting patient care and ensuring accurate communication among emergency medical services. Follow these steps to fill out the form thoroughly and accurately.
Once all sections are filled out, review the form for accuracy. Ensure that all signatures are obtained where necessary. This report will be crucial for billing, patient care continuity, and legal documentation.